Stricture Urethra
Stricture Urethra The urethra is the soft tube that allows urine to be passed out of the bladder. In men, the urethra is a thin tube like structure that starts from the lower opening of the bladder and traverses the entire length of the penis. It measures 21 cm in men. In women, it is a shorter tube coming off the lower opening of bladder and is between 2.5 to 4 centimeters (cm)
in length. The urethra has a sphincter that is normally closed to keep urine inside the bladder. When bladder fills with urine, there are both voluntary and involuntary controls to open the urethral sphincter to allow urine to come out.
Urethral stricture refers to any narrowing of the urethra for any reason whether or not it actually impacts the flow of urine out of the bladder. Any inflammation of urethra can result in scarring, which then can lead to a stricture or a narrowing of the urethra. Trauma, infection, tumors, surgeries, or any other cause of scarring may lead to urethral narrowing or stricture. Urethral stricture is significantly more common in men and boys compared to women and girls.
The following are common causes of scarring or narrowing of the urethra:
Some of the possible symptoms and complications of urethral stricture include the following:
Ultrasonogrphy: Ultrasound scan of the bladder is done to asses the effects of the stricture on the urinary system. So it is an indirect test to diagnose the stricture or bladder out flow obstruction. Scan may show residual urine in bladder, urine retention, bladder wall thickening, dilatation of the kidney and ureter.
Urethrography: A retrograde urethrogram is a routine radiologic procedure used to image the urethra. Hence a retrograde urethrogram is essential for diagnosis of urethral stricture. The procedure involves pushing of 20 ml of radiographic contrast by a syringe in to the urethra and a plain radiograph is obtained. Stricture urethra is seen as a segmental narrowing in caliber of the urethral lumen of varying length.
Uroflowmetry: Uroflowmetry is a diagnostic test done to check for abnormalities in the amount or flow rate of a patient’s urine. The procedure is straightforward and painless, and simply involves urinating into a funnel device attached to an electronic meter. It measures rate of flow of urine in ml/sec. Less than the normal flow rates indicates obstruction to flow of urine. Doctors commonly use uroflowmetry to check for possible bladder obstructions, urethral stricture, prostate enlargement, and bladder problems.
Cystoscopy: Cystoscopy is endoscopy of the urinary bladder via the urethra. It is carried out with a cystoscope under anesthesia in the operation theater.. The cystoscope is inserted into your urethra and stricture is visualized. Cystoscopy allows your doctor to look at areas of your bladder and urethra that usually do not show up well on X-rays. Tiny surgical instruments can be inserted through the cystoscope that allows your doctor to remove samples of tissue (biopsy) or samples of urine. Small bladder stones and some small growths can be removed during cystoscopy. This is done as a part of the treatment.
Surgery remains the only treatment for individuals with symptoms of urethral narrowing. Many surgical procedures are available for treating urethral strictures. Depending on the cause, type, severity of stricture and other medical and social aspects, the most appropriate procedure may be recommended for each individual case. The common procedures include
It is a commonly attempted simple technique for treating urethral strictures. This procedure is done under local or general anesthesia. Thin rods of increasing diameters are gently inserted into the urethra from the tip of the penis (meatus) in order to open up the urethral narrowing without causing any further injury to the urethra. This procedure may need to be repeated from time to time, as strictures may recur. The shorter the stricture, the less likely it is to recur after a dilation procedure. Occasionally, patients are given instructions and dilation instruments like a urethral catheter, lubricating gel, to perform the urethral dilation at home as needed.
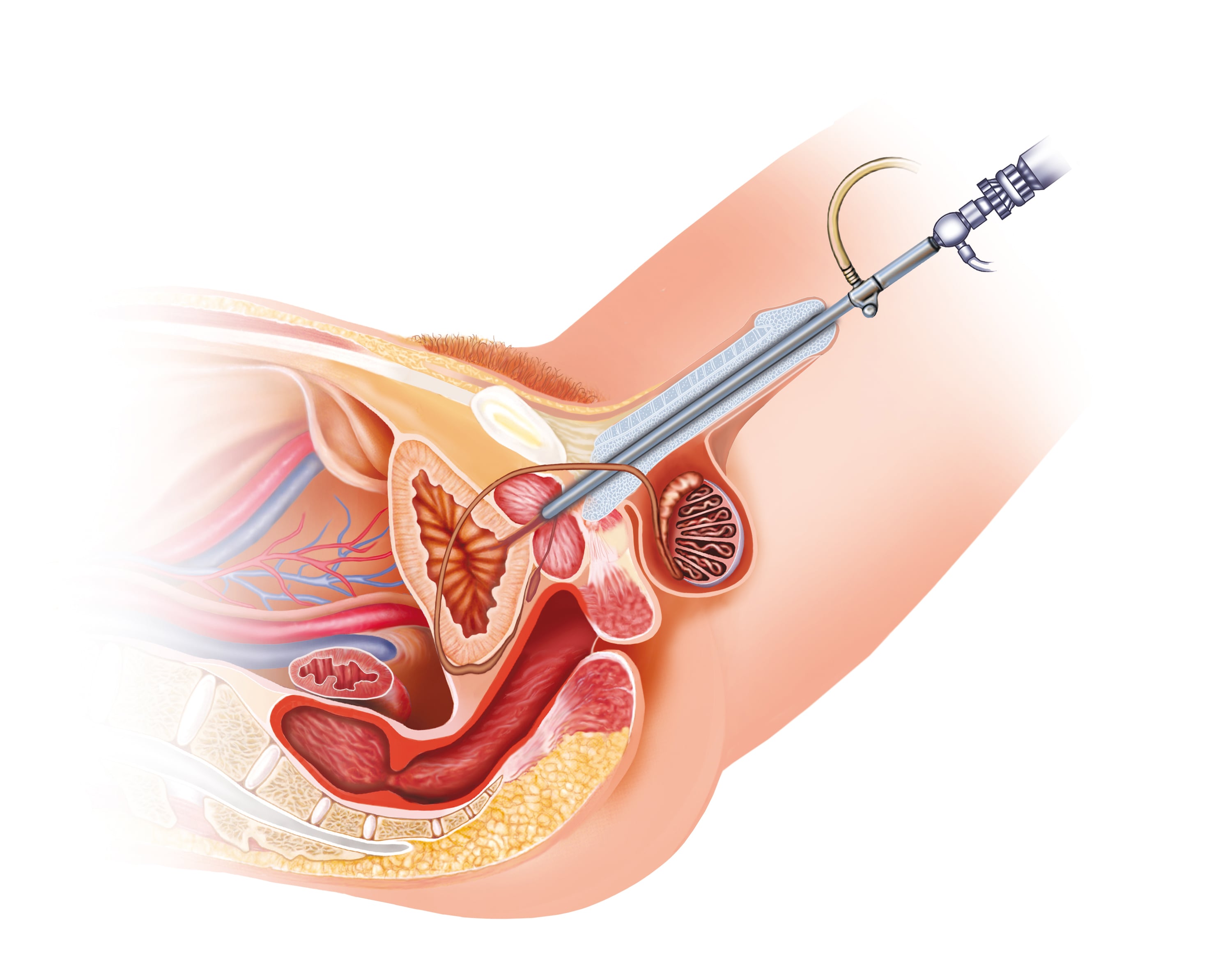
The surgical technique of “Urethrotomy” creates a widening of the urethra by sharp cutting using a special instrument. The operation is performed endoscopically through the external urinary meatus. There are two types of Urethrotomy:
Urethroplasty is an open surgical procedure for urethral reconstruction to treat urethral stricture. It can be performed by 2 methods; primary repair which involves complete excision of the narrowed part of the urethra. The proximal and distal patent parts are then rejoined. The second method of Urethroplasty utilizes tissue transfer or free graft technique. In this method, tissue is grafted from foreskin or buccal mucosa and is used to enlarge the strictured (narrowed) segment of the urethra. Urethroplasty is performed under general anesthesia. Two urethroplasty techniques are popularly used:
The Johansen’s procedure sometimes referred to as “Johansen’s urethroplasty” is a two stage procedure which was originally designed as a surgical repair for hypospadias. This is done long stricture, recurred strictures, BXO strictures, recurred after repeated surgeries. Urethra is opened all along its ventral length and laid open for six months or more. Once it is suitable urethra is re constructed back.
Placement of stents in to urethra to keep the lumen open was started many years back but discontinued because of poor outcomes.

Dr Mahendra Jain is an eminent and an extremely experienced Urologist ...
Read MoreCall Us
Conceptualized, Marketed & Promoted by Appadd India Pvt Ltd | Sitemap | Privacy Policy | Terms And Conditions | About Bangalore